Pay-Per-Call for Medicare: AEP Calls, Payouts & CMS Compliance (2026)
Pay per call Medicare explained for 2026: how Medicare inbound calls are generated and routed, the AEP and OEP demand cycle, how callers are qualified, why payouts are among the highest, and the CMS plus TCPA compliance layer that makes Medicare unique.

Rafael Hernandez
Founder & CEO
Ex-Microsoft SWE · $10M+ PPL ad spend
I hope you enjoy reading this blog post. If you want to try Lead Distro AI for free, click here.
Author: Rafael Hernandez | Founder & CEO of Lead Distro AI
Pay per call Medicare is the inbound-call monetization model for the Medicare market: a publisher generates a live phone call from a senior shopping for a Medicare Advantage or Medicare Supplement plan, a tracking number routes that caller to a licensed agent or call center, and the buyer pays a fixed price once the call passes a duration and qualification threshold. Because the prospect is already on the phone with active intent, this model converts faster than data leads, and Medicare is the classic high-volume, high-payout vertical of pay-per-call. It is also the most heavily regulated. On top of the federal Telephone Consumer Protection Act (TCPA) that governs every calling vertical, the Centers for Medicare and Medicaid Services (CMS) layers its own marketing rules on Medicare calls, including a required disclaimer and mandatory call recording.
This guide explains how Medicare pay per call leads are generated and routed, the enrollment-season demand cycle that drives the entire calendar, what Medicare callers are qualified on, why payouts run so high, and the CMS plus TCPA compliance stack you must respect. It closes with an honest comparison of pay per call against shared and exclusive Medicare data leads. To route Medicare inbound calls with AI scoring, see Lead Distro AI, or watch routing and ping-post bidding work end to end in the product tour.
Key Takeaways
- Pay per call Medicare bills per qualified inbound call, not per form fill, so the buyer pays only when a live senior clears a duration and pre-qualification threshold, which shifts the risk to call quality instead of contact rate.
- The Medicare calendar is built around enrollment seasons: the Annual Enrollment Period (AEP) runs October 15 to December 7 and is the peak demand window, while the Medicare Advantage Open Enrollment Period (OEP) runs January 1 to March 31 as a secondary cycle.
- Medicare callers are qualified on age, location, and plan status: age 65 or older (or under 65 with a qualifying disability), county of residence since Medicare Advantage plans are county-specific, and current coverage status.
- Medicare payouts are among the highest in pay per call because each enrolled member carries recurring plan value over time, so a single Medicare call is worth far more to a buyer than a typical auto or home call.
- CMS compliance is the differentiator and the liability: Medicare marketing calls require the CMS TPMO disclaimer and must be recorded and retained, on top of the TCPA prior express written consent standard.
- Routing, billing, and tracking run on a distribution platform using Round Robin, Weighted, Priority/Waterfall, or Ping-Post, with usage-based call tracking layered on the flat subscription.
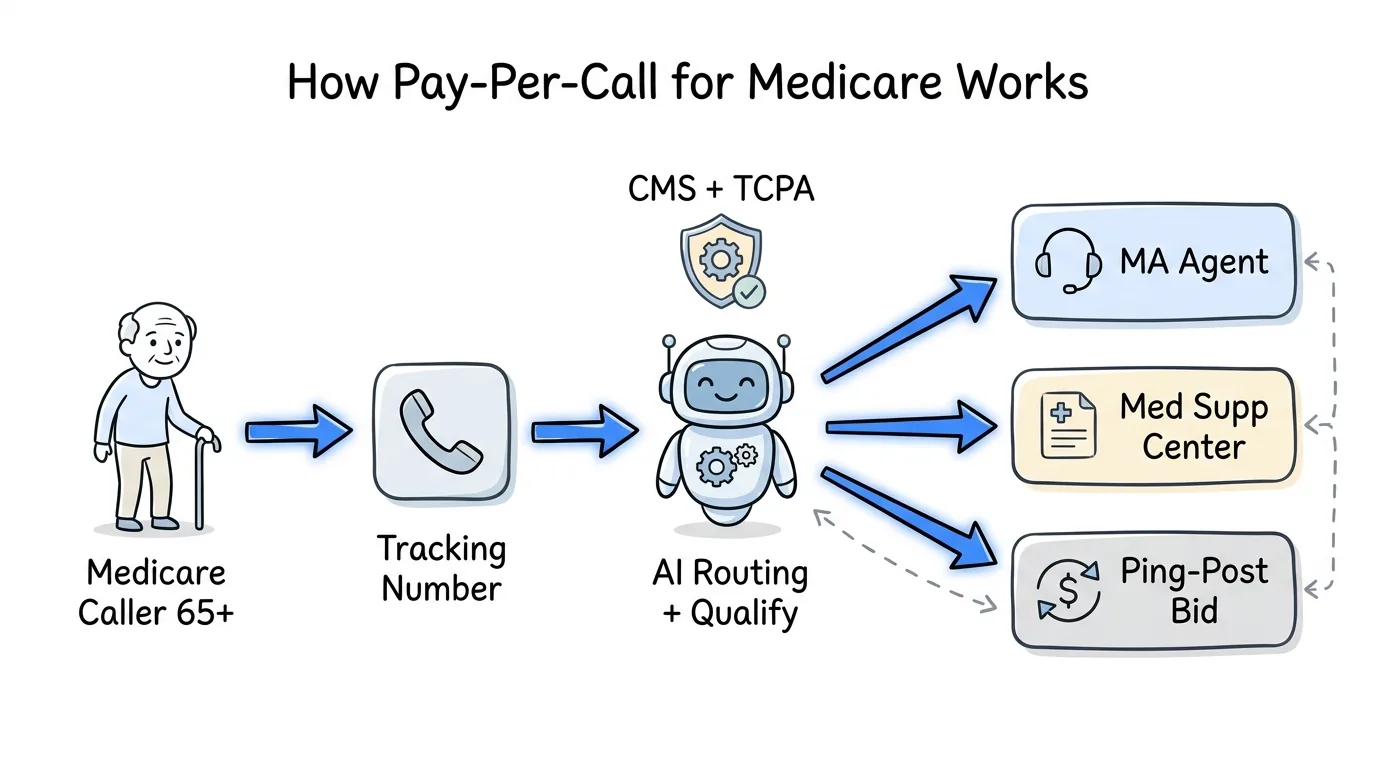
How Pay-Per-Call Works for Medicare
Pay per call inserts a tracked phone number between a publisher and a buyer. The publisher runs a Medicare campaign, a Google search ad for "Medicare Advantage plans," a Medicare plan comparison page, or a quote site, and displays a tracking number. When a senior calls, the platform's Dynamic Number Insertion (DNI) ties the call to its source, scores it, and routes the live caller to a buyer based on rules the buyer set: county, plan type, time of day, and bid.
The buyer pays only when the call clears a threshold, usually a minimum connected duration plus any interactive voice response (IVR) pre-qualification answers. That billable event protects buyers from junk calls and pushes publishers to send genuinely interested seniors. The result is a marketplace where Medicare agencies buy live intent at a known unit cost, and pay-per-call agencies monetize Medicare call inventory across multiple buyers without managing the enrollment themselves. Because Medicare is seasonal and county-specific, routing precision matters more here than in any other vertical.
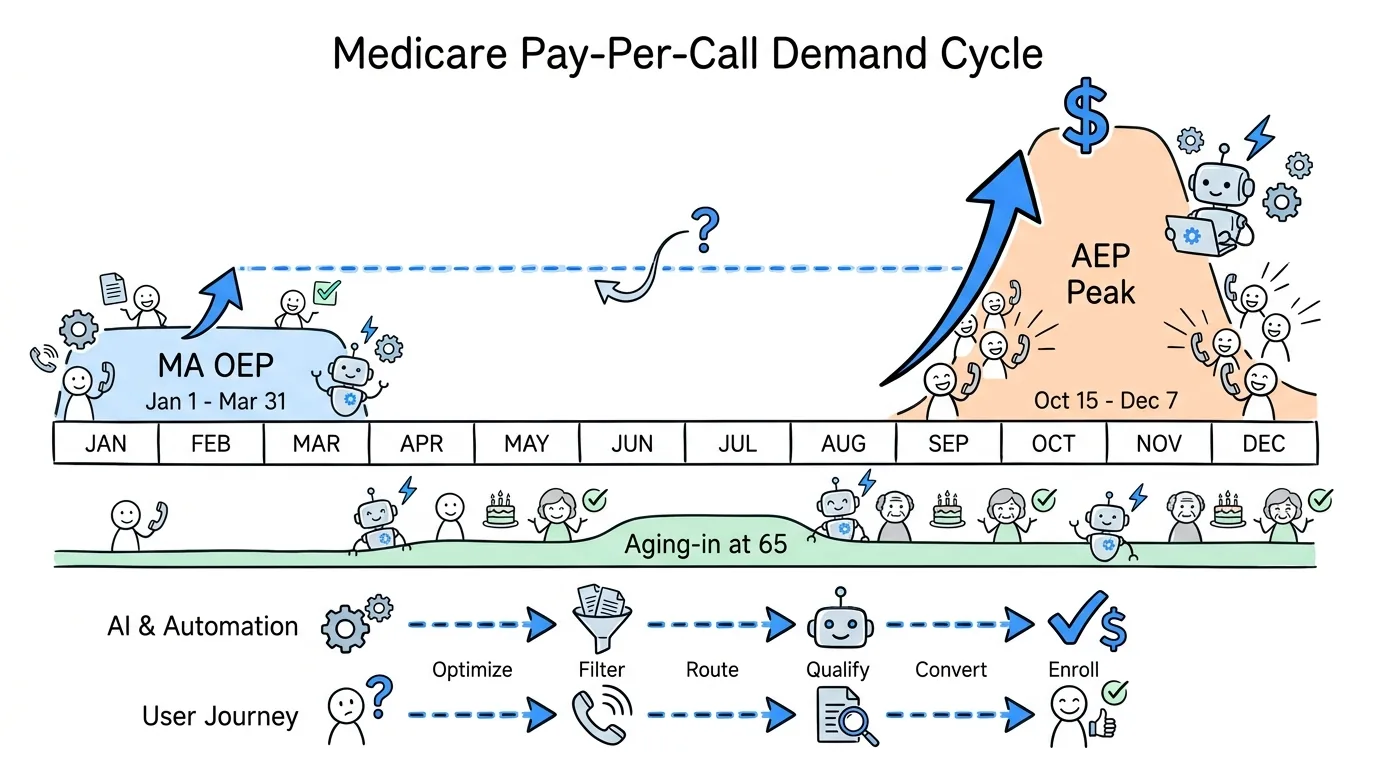
The Medicare Enrollment Season Demand Cycle
Medicare demand is not year-round. It concentrates into defined enrollment windows set by CMS, and the entire pay-per-call calendar bends around them. Understanding the seasons is the difference between paying for calls when buyers are desperate for them and paying when no one is enrolling.
Annual Enrollment Period (AEP)
The Annual Enrollment Period runs October 15 to December 7 every year, and during it any Medicare beneficiary can join, switch, or drop a Medicare Advantage or Part D plan (Medicare.gov, Joining a plan). AEP is the Super Bowl of Medicare marketing. Call volume and payouts both peak, agent capacity is maxed, and publishers compete hard for placement. Most of a Medicare pay-per-call book's annual revenue is earned in these eight weeks, which is why buyers raise bids and loosen caps to absorb every qualified call they can answer live.
Medicare Advantage Open Enrollment Period (OEP)
The Medicare Advantage Open Enrollment Period runs January 1 to March 31. During OEP, beneficiaries already enrolled in a Medicare Advantage plan can switch to a different Advantage plan or drop back to Original Medicare (Medicare.gov, Joining a plan). OEP is a smaller, secondary cycle compared to AEP, but it keeps call inventory liquid in the first quarter. Outside AEP and OEP, demand is driven mainly by Special Enrollment Periods and people newly aging into Medicare at 65, a steadier but thinner stream that publishers use to keep the lights on between seasons.
How Medicare Callers Are Qualified
Medicare buyers do not pay for any inbound senior. They pay for callers who match the criteria that make an enrollment possible, and those criteria are tighter than most verticals because eligibility and plan availability are rule-bound. The standard Medicare pay per call qualification filters are:
- Age and eligibility. The caller is 65 or older, or under 65 and Medicare-eligible through a qualifying disability or condition. This is the gate, since a 60-year-old shopping early cannot enroll yet.
- County of residence. Medicare Advantage plans are sold and priced by county, so a call only has value if the caller lives in a county where the buyer's plans are available. A correct ZIP-to-county match is non-negotiable.
- Current plan status. Whether the caller has Original Medicare, an existing Advantage plan, or no coverage yet decides which enrollment window applies and which products the agent can offer.
- License and product match. The agent must be licensed in the caller's state and appointed with carriers that serve that county. Routing a call to an unappointed agent wastes spend and creates compliance risk.
An original insight from running mixed call-and-lead operations: in Medicare, the most expensive mistake is not a low billable rate, it is a county mismatch that surfaces after the agent is already on the phone. Auto or home calls tolerate a loose state match; Medicare does not, because the plans themselves do not exist outside the county. The publishers who win Medicare margin are the ones who qualify county before transfer, not after, so the buyer never burns a paid call on a senior they legally cannot enroll.
CMS Compliance for Medicare Pay-Per-Call
Medicare is the most regulated vertical in pay per call, and the reason is a second federal layer that no other line carries. Auto, home, and most other calls answer only to the TCPA. Medicare answers to the TCPA and to CMS marketing rules at the same time. Getting this wrong is a real liability, not a paperwork nuisance, so treat compliance as a buying decision.
The CMS TPMO Disclaimer
CMS treats most lead generators, marketers, and agencies in the Medicare space as Third-Party Marketing Organizations (TPMOs). A TPMO that does not offer every plan in an area must state the standard CMS disclaimer: "We do not offer every plan available in your area. Any information we provide is limited to those plans we offer in your area. Please contact Medicare.gov or 1-800-MEDICARE to get information on all of your options." The disclaimer must appear on marketing materials and be communicated verbally on Medicare sales and marketing calls before plan benefits are discussed, and it must be used verbatim (Ritter Insurance Marketing, Medicare compliance). A version that names the exact number of organizations and plans represented is required once a beneficiary's location is known. Always confirm the current wording and timing with CMS for the active plan year before scripting it.
Mandatory Call Recording
CMS requires TPMOs to record Medicare marketing, sales, and enrollment calls with beneficiaries in their entirety, covering both inbound and outbound calls that could lead to enrollment, and to retain them. Retention rules are not uniform: enrollment records must be kept for ten years, while marketing call audio and transcripts carry their own retention windows (Ritter Insurance Marketing, Medicare compliance). For a pay-per-call operation, this means recording and retention cannot be bolted on after the fact. Every Medicare call path has to capture and store the recording from the first connected second, which is one more reason routing and tracking should run on infrastructure built for it.
The TCPA Layer
Underneath the CMS rules sits the TCPA, which governs every telemarketing call. The TCPA requires prior express written consent before autodialed, prerecorded, or artificial-voice telemarketing calls and texts, and restricts calls to numbers on the National Do-Not-Call Registry (FCC, Telemarketing and Robocalls). One development is widely misreported, so state it accurately: the FCC's 2023 one-to-one consent rule, which would have required separate consent for each individual seller, was vacated by the U.S. Court of Appeals for the Eleventh Circuit in Insurance Marketing Coalition Ltd. v. FCC on January 24, 2025, before it took effect (Eleventh Circuit decision coverage, Kelley Drye). The pre-existing prior-express-written-consent standard remains in force, so capture and retain per-lead consent records and scrub Do-Not-Call lists. This is general information, not legal or compliance advice; confirm the current CMS marketing rules and TCPA requirements with qualified counsel each plan year.
Medicare Pay-Per-Call vs Shared and Exclusive Medicare Leads
Pay per call is one of three ways to buy Medicare demand, and each fits a different operation. The table compares them on what you receive, contact speed, cost structure, and who owns the prospect record.
| Buying Model | What You Get | Speed to Contact | Cost Structure | Prospect Record |
|---|---|---|---|---|
| Pay Per Call | Live inbound Medicare caller, billed per qualified call | Instant, caller is already on the phone | Higher per unit, paid only on billable calls | Buyer does not own the record |
| Shared Medicare Data Leads | Form fill sold to several buyers | Slow, you dial and compete | Cheapest per lead, low contact rate | Shared across buyers |
| Exclusive Medicare Data Leads | Form fill sold to one buyer | Slow, you dial first | Highest per lead, you own follow-up | Buyer owns the record |
Pay per call wins on speed and intent during enrollment season, when every minute of AEP counts and a senior already on the phone is worth more than ten form fills you have to chase. Shared data leads are cheap but contact rates suffer because the senior fields several calls at once. Exclusive data leads cost the most per record but let an agency own the relationship and nurture across enrollment periods, which suits a CRM-driven Medicare book. The strongest Medicare operations run pay per call for high-intent AEP and OEP volume and exclusive data leads for year-round nurture of seniors aging in at 65, distributing both from one platform so the P&L is unified. For a deeper breakdown of buying and routing form leads, read our Medicare leads guide. Comparing verticals? See pay-per-call for solar and pay-per-call for legal, two more high-payout call categories.
Routing, Billing, and Tracking With Lead Distro AI
Once Medicare calls are flowing, the platform layer decides who gets each call, how it bills, and how it is tracked. Lead Distro AI handles Medicare pay-per-call with four distribution methods:
- Round Robin spreads calls evenly across a buyer pool so no single agent is starved or flooded during an AEP rush.
- Weighted sends a higher share of calls to your best-converting or highest-paying Medicare buyers.
- Priority/Waterfall offers each call to the top buyer first and falls down the list if they decline or are capped (the same model often called a waterfall).
- Ping-Post broadcasts the call's qualifying attributes, county, age band, plan status, to multiple buyers in real time, collects bids, and routes the live caller to the highest bidder, the revenue-maximizing model for high-payout lines like Medicare.
Every inbound call is scored with AI before routing, so buyers receive pre-qualified seniors rather than raw inbound volume, and county can be matched before transfer rather than after billing. Tracking runs on Dynamic Number Insertion, attributing each call to its publisher and campaign, and billing is reconciled per buyer in real time with P&L by source. On pricing: the platform subscription starts at $299 per month flat. Call tracking is billed separately and is usage-based, a per-tracking-number monthly fee plus a per-minute rate for inbound calls, layered on top of the subscription. A 7-day free trial is available with a credit card required. To see ping-post bidding in a Medicare workflow, start your free trial or read the insurance vertical overview. For the broader insurance picture, see our pay-per-call for insurance overview and best ping-post software for insurance guide. New to the model? Start with what is pay per call and how to start a pay-per-call agency.
FAQ
What is pay per call for Medicare?
Pay per call for Medicare is an inbound-call model where a publisher generates a live phone call from a senior shopping for a Medicare Advantage or Medicare Supplement plan, a tracking number routes the caller to a licensed agent or call center, and the buyer pays a fixed price once the call clears a duration and pre-qualification threshold. Because the prospect is already on the phone with intent, it converts faster than data leads. Medicare is one of the highest-payout pay-per-call verticals, and the most regulated, since CMS marketing rules apply on top of the TCPA.
When is the peak season for Medicare pay per call leads?
The peak is the Annual Enrollment Period (AEP), which runs October 15 to December 7, when any Medicare beneficiary can join, switch, or drop a Medicare Advantage or Part D plan. Call volume and payouts both spike during these eight weeks, and most of a Medicare pay-per-call book's annual revenue is earned then. A secondary window, the Medicare Advantage Open Enrollment Period (OEP), runs January 1 to March 31 and lets existing Advantage members switch plans. Outside these windows, demand comes mainly from people newly aging into Medicare at 65 and Special Enrollment Periods.
How are Medicare inbound calls qualified?
Medicare callers are qualified on age and eligibility (65 or older, or under 65 with a qualifying disability), county of residence since Medicare Advantage plans are sold and priced by county, current plan status, and a license and carrier match so the agent can actually enroll the caller. County matching is the critical filter unique to Medicare, because the plans themselves do not exist outside the county. Qualifying county before transfer rather than after is the single biggest driver of Medicare pay-per-call margin.
What CMS compliance rules apply to Medicare pay per call?
CMS treats most Medicare lead generators and agencies as Third-Party Marketing Organizations (TPMOs). TPMOs must state the standard CMS disclaimer on marketing materials and on sales and marketing calls before plan benefits are discussed, and must record Medicare marketing, sales, and enrollment calls with beneficiaries and retain them, with enrollment records kept for ten years. These rules sit on top of the TCPA. This is general information, not legal advice; confirm the current CMS marketing rules each plan year with qualified counsel.
Is Medicare pay per call TCPA compliant?
Medicare pay per call can be fully TCPA compliant when consent and Do-Not-Call rules are followed. The TCPA requires prior express written consent for autodialed or prerecorded telemarketing calls and texts and restricts calls to numbers on the National Do-Not-Call Registry. The FCC's 2023 one-to-one consent rule was vacated by the Eleventh Circuit in January 2025 and never took effect, so the prior written-consent standard governs. On Medicare specifically, layer CMS recording and disclaimer obligations on top. Retain per-lead consent records and scrub DNC lists. This is general information, not legal advice.
How do I route and bill Medicare calls?
Medicare calls are routed and billed on a distribution platform. Lead Distro AI supports Round Robin, Weighted, Priority/Waterfall, and Ping-Post distribution, scores each call with AI before routing, matches county before transfer, and attributes calls with Dynamic Number Insertion. The platform subscription starts at $299 per month flat, and call tracking is usage-based on top of that, a per-number monthly fee plus a per-minute inbound rate. A 7-day free trial is available with a credit card required.
Conclusion
Medicare is the classic pay-per-call vertical: high volume during AEP, payouts among the highest of any line, and a demand cycle you can plan a whole year around. It is also the one that punishes sloppiness, because CMS marketing rules sit on top of the TCPA, and a county mismatch or a missing disclaimer is not a rounding error. The economics turn on qualifying county and eligibility before routing, documenting consent under the current TCPA standard, recording and retaining Medicare calls per CMS, and routing each call with the method that fits, with Ping-Post earning the most on high-payout Medicare inventory.
If you want to run Medicare calls and data leads from one dashboard with AI scoring, county matching, and real-time P&L, start your free 7-day trial and route your first call before AEP opens. See the insurance vertical page for the full feature set, or take the product tour to watch ping-post bidding work end to end.
Building a Medicare pay-per-call book before AEP? Start your 7-day free trial and see how Lead Distro AI scores, qualifies county, routes, and bills Medicare Advantage and Medicare Supplement calls from one platform. Credit card required.
About the Author
Founder & CEO of Lead Distro AI & Great Marketing AI
UC Berkeley graduate and former software engineer at Microsoft. Rafael built Lead Distro AI after managing over $10M in ad spend for performance marketing agencies (pay-per-lead and pay-per-call), including running campaigns for Neil Patel. He combines deep software engineering expertise with hands-on performance marketing experience to build tools that help these agencies scale profitably.
About Lead Distro AI
Lead Distro AI: AI-Powered Lead Distribution & Call Tracking That Maximizes ROI
The modern platform for pay-per-lead and pay-per-call agencies. Route, score, and deliver leads with AI-powered automation and real-time P&L tracking. Built for performance marketing agencies and lead buyers across legal, insurance, mortgage, solar, and home services verticals.
4 Distribution Methods
Waterfall, Round Robin, Weighted, Ping-Post
Ping-Post Auctions
Real-time bidding with sub-second routing
Real-Time P&L Reporting
Track revenue, costs, and profit per campaign
Call Tracking
Assign tracking numbers, record calls, and attribute conversions
AI Lead Scoring
Score every lead before routing to maximize conversion
Partner Portal
Self-serve dashboard for buyers to track leads